Navigating Interventions
 Navigating Interventions: An exploration of genetic and medical interventions during conception, pregnancy, and labor, navigating the ethical considerations, long-term impacts, and strategies for informed decision-making and advocacy within the community.
Navigating Interventions: An exploration of genetic and medical interventions during conception, pregnancy, and labor, navigating the ethical considerations, long-term impacts, and strategies for informed decision-making and advocacy within the community.
Understanding Genetic Interventions: Genetic interventions during the pre-conception stage and pregnancy, including genetic testing and counseling, examining their implications and considerations for individuals and families.
Ethical Implications of Genetic Interventions: The complex ethical terrain surrounding genetic interventions, exploring their impact on informed decision-making, autonomy, and the broader societal implications of genetic manipulation.
Medical Interventions during Conception, Pregnancy, and Labor: Exploring the spectrum of medical interventions utilized during conception, pregnancy, and labor, including IVF, C-sections, and medical relief practices, considering their long-term implications and ethical considerations.
Understanding IVF, C-sections, and Medical Relief Practices: Examining the rationale, procedures, and outcomes associated with IVF, C-sections, and medical relief practices during labor, fostering understanding and informed decision-making among individuals and communities.
Ethical Decision-Making in Interventions: Discussing ethical decision-making in the context of genetic and medical interventions, considering principles of autonomy, beneficence, non-maleficence, and justice, and advocating for patient-centered care and informed consent.
Community Implementation:
Advocating for Informed Decision-Making: Developing strategies to advocate for informed decision-making and ethical considerations in genetic and medical interventions, empowering individuals and communities to make choices aligned with their values and preferences.
Raising Awareness and Advocating for Policies: Launching campaigns to raise awareness about genetic and medical interventions, their impact, and ethical considerations, advocating for policies that prioritize patient education, autonomy, and informed consent in healthcare interventions.
 Navigating Interventions en 1
Navigating Interventions en 1
Navigating Interventions en 2 (Cesarean)

Παρεμβάσεις από την περίοδο πριν από την σύλληψη μέχρι τον τοκετό 1
Παρεμβάσεις από την περίοδο πριν από την σύλληψη μέχρι τον τοκετό 2

Amniocentesis is a surgical technique that has been used for a variety of indications. The procedure was first utilized in Germany in the early 1880s to treat polyhydramnios (Lambl, 1881; Schatz, 1882). In 1930, Menées et al. (1930) used amniocentesis to inject contrast media into the amniotic sac in order to evaluate the fetus and localize the placenta. The procedure of using amniocentesis to introduce hypertonic saline into the amniotic sac for pregnancy termination made its appearance in 1937 (Aburel, 1937). Amniocentesis utilization increased rapidly in the 1950s, when spectrophotometric analysis of bilirubin proved valuable in monitoring fetuses with Rh isoimmunization (Bevis, 1952; Walker, 1957). (Elias, S., Simpson, J.L. (1986). Amniocentesis. In: Milunsky, A. (eds) Genetic Disorders and the Fetus. Springer, Boston, MA. https://doi.org/10.1007/978-1-4684-5155-9_2)
Amniocentesis: …There is an increased rate of sample contamination (statistically significant) when using 21 G needle sizes and a significant difference in contamination between primiparous and multiparous patients, with contamination being more frequent in multiparous patients. The use of Doppler ultrasonography may benefit the procedure, as the contamination rate was significantly reduced when used during amniocentesis.
Ciortea, Razvan et al. “Amniocentesis-When It Is Clear That It Is Not Clear.” Journal of clinical medicine vol. 12,2 454. 6 Jan. 2023, doi:10.3390/jcm12020454
ALSO Read the following paper (Jindal A, Sharma M, Karena ZV, et al. Amniocentesis. [Updated 2023 Aug 14]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK559247/):
…Both maternal and fetal complications can occur with amniocentesis.

Maternal Complications
-
There is an estimated 2.6% risk of fetomaternal hemorrhage.
-
Maternal isoimmunization in Rh-negative cases.
-
There is minimal chance of introducing skin bacteria into the amniotic cavity. The risk of chorioamnionitis and uterine infections is less than 0.1%.
-
The procedure increases the risk of preterm labor in the third-trimester amniocentesis. Preterm premature rupture of membrane and oligohydramnios are common complications encountered following amniocentesis.
-
There is a 2% to 3% risk of vaginal bleeding.
-
Post-procedure pain and maternal discomfort: Mean pain intensity described is 1.6+/-1.3 when noted on a scale of 0 to 7.[35]
-
Amniotic fluid embolism, very rare
-
There can be hematoma of maternal skin or intestinal or internal organ injuries.
Fetal Complications
-
On average, the fetal loss rate associated with amniocentesis is 0.11%. The loss is 0.56% within 28 days and 0.09% within 42 days.[29]
-
The risk of fetal loss is higher in women who are otherwise at a higher risk of miscarriage, such as women carrying fetuses with structural malformations, fibroids, obese women, and women with vaginal infections at the time of the procedure. Amniocentesis in up to 86.0% of the patients is safe and free from complications.[36] The risk of fetal loss in case of multiple pregnancies is higher.
-
-
Amniotic fluid leak: 1% to 2%, and usually associated with spontaneous sealing of membranes.[29] It may also result in:
-
Fetal lung hypoplasia
-
Respiratory distress
-
-
Fetal injuries like bleeding from the cord, ocular injuries, and postural deformities like talipes equinovarus (clubfoot) might occur.
-
The risk of complications is high when more than or equal to 3 pricks are used to obtain amniotic fluid. In ideal conditions, if an adequate fluid sample is not obtained in two pricks, the procedure should be abandoned for 24 hours, after which it can be re-attempted. The risk is less in experienced hands, i.e., people who perform more than 300 procedures/year.
-
EPISIOTOMY (PERINEOTOMY)
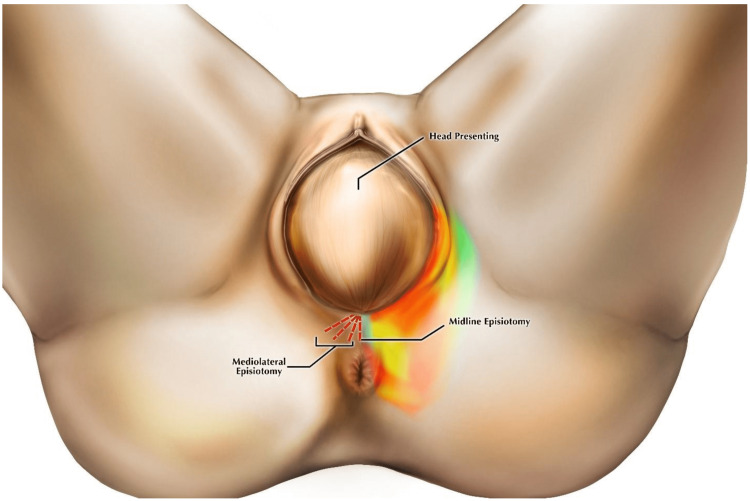 Episiotomy is the most commonly performed planned surgical incision on the perineum during the second stage of labour. Indications of episiotomy are foetal distress, complicated baby positions such as breeches, premature births, large babies, and vacuum delivery. Maternal benefits are reduced risk of perineal trauma, subsequent pelvic floor dysfunction and prolapse, urinary incontinence, faecal incontinence, and sexual dysfunction. Potential benefits for the foetus were thought to include a shortened second stage of labour as a result of more rapid and spontaneous delivery. It can also result in adverse consequences of episiotomy, including an extension to a third- or fourth-degree tear, anal sphincter dysfunction, and dyspareunia.
Episiotomy is the most commonly performed planned surgical incision on the perineum during the second stage of labour. Indications of episiotomy are foetal distress, complicated baby positions such as breeches, premature births, large babies, and vacuum delivery. Maternal benefits are reduced risk of perineal trauma, subsequent pelvic floor dysfunction and prolapse, urinary incontinence, faecal incontinence, and sexual dysfunction. Potential benefits for the foetus were thought to include a shortened second stage of labour as a result of more rapid and spontaneous delivery. It can also result in adverse consequences of episiotomy, including an extension to a third- or fourth-degree tear, anal sphincter dysfunction, and dyspareunia.
More below Choudhari, Rutuja G et al. “A Review of Episiotomy and Modalities for Relief of Episiotomy Pain.” Cureus vol. 14,11 e31620. 17 Nov. 2022, doi:10.7759/cureus.31620:
Related to consent:
Women do not experience consent for episiotomy as consistently informed and voluntary. Nor do they have a sense of genuine choice. Information provision, particularly regarding the risks of and alternatives to episiotomy, was thought to be inhibited by practical factors including time pressure, concern for the baby’s health and women’s state of exhaustion. Brief discussions around episiotomy, at a point where there was ostensibly no alternative, suggest that the current episiotomy consent process fails to promote a dialogue in which women’s choice-making is prioritised.
Thus: Consent to episiotomy is not consistently informed and voluntary and more often takes the form of compliance. Information must be provided to women in a more timely fashion in order to fulfil legal requirements, and to facilitate a sense of genuine choice. Read Djanogly, T., Nicholls, J., Whitten, M. et al. Choice in episiotomy – fact or fantasy: a qualitative study of women’s experiences of the consent process. BMC Pregnancy Childbirth 22, 139 (2022). https://doi.org/10.1186/s12884-022-04475-8
ALSO: Bączek, G.; Rychlewicz, S.; Sys, D.; Rzońca, P.; Teliga-Czajkowska, J. Episiotomy for Medical Indications during Vaginal Birth—Retrospective Analysis of Risk Factors Determining the Performance of This Procedure. J. Clin. Med. 2022, 11, 4334. https://doi.org/10.3390/jcm11154334
ULTRASOUND
Though antenatal ultrasound was largely seen as positive, long-term adverse psychological and reproductive consequences were reported for some. Gender inequity may be reinforced by female feticide following ultrasound in some contexts. Provider attitudes and behaviours, time to engage fully with service users, social norms, access to follow up, and the potential for overuse all need to be considered. (Moncrieff, Gill et al. “First and second trimester ultrasound in pregnancy: A systematic review and metasynthesis of the views and experiences of pregnant women, partners, and health workers.” PloS one vol. 16,12 e0261096. 14 Dec. 2021, doi:10.1371/journal.pone.0261096). Also other studies link to low birth weight, delayed speech, dyslexia, and non–right-handedness.
EPIDURAL
Both local anesthetics and opioids can cross the placenta and can be detected in the umbilical vein and neonatal urine after delivery.These drugs may accumulate and lead to neonatal depression due to ion-trapping in the more acidic fetal circulation and impaired clearance due to immature liver enzymes. Epidural is associated with a reduction in uterine artery blood flow during contractions, even when using low concentrations of local anesthetic. (, , . Epidural analgesia in labor: A narrative review. Int J Gynecol Obstet. 2022; 159: 356–364. doi:10.1002/ijgo.14175)
Forceps delivery complications
Forceps delivery complications may happen when medical providers apply too much force onto a baby’s head when using forceps to assist with delivery.
Injury from forceps delivery include:
- Intracranial hemorrhage, a severe condition where bleeding occurs inside the skull
- Nerve damage causing temporary facial nerve palsy (drooping or weakness) that heals within a few weeks
- Severe brain injury leading to long-term neurological complications or developmental delays
- Skull fractures that heal on their own and don’t cause long-term damage
- Surface wounds to the face or head that heal in a few daysVacuum extractor complications
Injury from Vacuum extraction happen when delivery teams fail to use extractors properly during vaginal delivery.
Complications from vacuum extractors include:
- Cephalohematomas
- Facial nerve injuries and palsies
- Retinal (eye) hemorrhage
- Scalp lacerations
BIRTH INJURIES
Common early signs of many types of birth injuries include:
- Abnormal appearance: Look for any unusual physical features or signs of distress, such as bluish or pale skin tone
- Developmental delays: Watch for any milestones your child does not reach on time
- Difficulty breathing: Newborns may struggle to breathe if they’ve experienced a birth injury
- Excessive crying: Persistent crying could indicate discomfort or pain due to an injury
- Feeding problems: Difficulty with nursing or bottle-feeding can be a sign of injury
- Limited movement: Several types of birth injuries may restrict a newborn’s ability to move certain body partshe most common types of birth injuries?There are several types of birth injuries. Learn more about common birth injury types below.
-
- Brachial plexus injury and Erb’s palsy
- Brain damage
- Cephalohematoma (skull bleeding)
- Cerebral palsy
- Forceps delivery complications
- Hydrocephalus
- Hypoxic-ischemic encephalopathy (HIE)
- Infant meningitis
- Kernicterus
- Meconium aspiration syndrome (MAS)
- Periventricular leukomalacia (PVL)
- Shoulder dystocia
- Spinal cord injuries
- Stillbirth (intrauterine fetal demise)
- Vacuum extractor complications
-
- In addition to the more common types of birth injuries already mentioned, there are several other forms of birth trauma that can affect delicate newborns.These other birth injury types may occur during childbirth:
- Caput succedaneum: Fluid buildup or swelling on the scalp
- Cervical dystonia: Contraction of neck muscles causing involuntary turning of the head
- C-section injuries: Harm caused during cesarean deliveries
- Facial paralysis: Loss of facial muscle movement
- Hematoma: Blood accumulation in a tissue
- Infant torticollis: Twisted neck
- Intraventricular hemorrhage: Blood accumulation in the brain
- Klumpke’s palsy: Nerve damage that affects the muscles of the arm
- Subconjunctival hemorrhage: Blood accumulation in the eye
ASPECTS OF BEING BORN CESAREAN by Olga Gouni
Medical Relief Practices
- Epidural Anesthesia provides effective pain relief during labor by blocking nerve impulses in the lower spinal region.
- Opioid Analgesics (e.g., Fentanyl) provide short-term pain relief during labor by blocking pain signals in the brain. Can cause drowsiness, respiratory depression in the baby, and potential dependency issues.
- Nitrous Oxide (Entonox) provides mild to moderate pain relief during labor through inhalation. It requires coordination and understanding of breathing techniques.
Social dimensions of preimplantation genetic diagnosis:a literature review (Lemke, T., & Rüppel, J. (2018). Social dimensions of preimplantation genetic diagnosis: a literature review. New Genetics and Society, 38(1), 80–112. https://doi.org/10.1080/14636778.2018.1549983)
Preimplantation genetic diagnosis (PGD) is a complex combination of reproductive techniques and genetic diagnostic procedures. Prior to establishing a pregnancy, embryos are created outside the human body using in vitro fertilization (IVF). In a second step, the embryos are screened for genetic and chromosomal characteristics using cytogenetic or molecular genetic diagnostic technologies. The purpose of genetic testing is to identify embryos that are free from a distinctive genetic or chromosomal alteration that may cause illness or disability.
Since it was first carried out successfully in 1990, PGD has generated a great deal of controversy both in public and in the academic world. Some observers in medicine and the social sciences and humanities have come to regard PGD as a new form of eugenics. According to this view, the selection of embryos prior to transfer marks a decisive threshold that goes beyond the option of terminating pregnancy subsequent to a prenatal diagnostic finding. The philosopher Jürgen Habermas, for example, has warned against “eugenic programming of desirable traits and dispositions”, which is morally reprehensible in that it “commits the person concerned to a specific life-project or, in any case, puts specific restrictions on his freedom to choose a life of his own” Read more:
Preimplantation Genetic Screening (PGS)
Women’s fecundity decreases gradually with increasing age, accompanied by significant increases in the rates of aneuploidy and spontaneous miscarriages [1]. These observations have led to the attractively logical hypothesis of preimplantation genetic screening (PGS), that the transfer of only euploid embryos should improve IVF outcomes, with older women considered as the best candidates. However, PGS, first proposed by Verlinsky and Kuliev in 1996, is a still unproven hypothesis… Read the paper (Gleicher, N., Orvieto, R. Is the hypothesis of preimplantation genetic screening (PGS) still supportable? A review. J Ovarian Res 10, 21 (2017). https://doi.org/10.1186/s13048-017-0318-3)
Ethical issues in new uses of preimplantation genetic diagnosis
PGD is increasingly available for aneuploidy in low prognosis IVF patients and for single gene mutations that cause genetic disease, susceptibility to cancer, and late onset disorders. If PGD is acceptable to prevent offspring with serious genetic disease, then these additional uses should be acceptable as well. There is also ethical support for using PGD to assure that a child is an HLA match with an existing child. More controversial is the use of PGD for gender selection, particularly for the first child. Equally controversial would be its use to screen embryos for hearing, sexual orientation, and other nonmedical traits—uses that are now highly speculative. Careful ethical analysis and open public debate is essential if new uses of PGD are to become acceptable methods for having children. Read the whole paper: John A. Robertson, Extending preimplantation genetic diagnosis: the ethical debate: Ethical issues in new uses of preimplantation genetic diagnosis, Human Reproduction, Volume 18, Issue 3, March 2003, Pages 465–471, https://doi.org/10.1093/humrep/deg100
Navigating Interventions Table
NEVER forget: negative emotional valence enhances recapitulation
Bowen, H.J., Kark, S.M. & Kensinger, E.A. NEVER forget: negative emotional valence enhances recapitulation. Psychon Bull Rev 25, 870–891 (2018). https://doi.org/10.3758/s13423-017-1313-9
Primitive Reflexes
Key laws and regulations related to genetic testing and interventions in Europe, the USA & elsewhere:
- Europe
In Europe, genetic testing and interventions are regulated under various laws and directives aimed at ensuring ethical standards, protecting privacy, and promoting public health. Some key regulations include:
- General Data Protection Regulation (GDPR): Although not specific to genetics, GDPR sets rules for the processing of personal data, including genetic data, within the European Union (EU). It emphasizes consent, transparency, and data protection rights for individuals.
- Directive 98/79/EC on in vitro diagnostic medical devices: This directive outlines requirements for genetic testing devices used in clinical settings, ensuring their safety, performance, and reliability. It also includes provisions for informed consent and quality assurance.
- Directive 2001/20/EC on clinical trials: This directive governs clinical trials in the EU, including those involving genetic testing. It establishes standards for patient protection, informed consent, and ethical review.
- European Convention on Human Rights and Biomedicine (Oviedo Convention): Although not an EU law, the Oviedo Convention, ratified by many European countries, provides ethical guidelines on biomedical research, genetic testing, and interventions. It emphasizes respect for human dignity, autonomy, and informed consent.
- USA
In the United States, genetic testing and interventions are regulated by federal and state laws aimed at protecting individuals’ rights, ensuring quality healthcare, and preventing discrimination. Key laws and regulations include:
- Genetic Information Nondiscrimination Act (GINA): GINA prohibits health insurers and employers from discriminating against individuals based on genetic information. It also restricts the collection and use of genetic information for employment and insurance purposes.
- Health Insurance Portability and Accountability Act (HIPAA): HIPAA includes provisions that protect the privacy and security of health information, including genetic information. It limits the disclosure of genetic information by healthcare providers and insurers.
- Clinical Laboratory Improvement Amendments (CLIA): CLIA regulates laboratory testing, including genetic testing, to ensure accuracy, reliability, and quality. Laboratories performing genetic tests must meet CLIA standards for proficiency testing, personnel qualifications, and quality control.
- Food and Drug Administration (FDA) Regulations: The FDA regulates genetic tests and medical devices through pre-market review and post-market surveillance. It ensures the safety and effectiveness of genetic tests marketed in the USA.
- Americans with Disabilities Act (ADA): ADA prohibits discrimination based on genetic information in employment and ensures individuals with genetic conditions are protected from discrimination in the workplace.
3. Asia
- Japan: Japan has guidelines on genetic testing and ethical considerations, including the Act on the Protection of Personal Information, which governs the use of genetic information.
- China: China has regulations on genetic research and testing, with guidelines from the Ministry of Health that cover ethical standards and patient consent.
India: India does not have specific national legislation on genetic testing but follows guidelines from the Indian Council of Medical Research (ICMR) and ethical standards for biomedical research
4. Africa
- South Africa: South Africa has guidelines on genetic research and testing, including ethical standards outlined by the National Health Research Ethics Council (NHREC).
- Nigeria: Nigeria has guidelines on genetic research and ethical standards, although specific legislation may vary by region.
5. Australia and Oceania
- Australia: Australia has guidelines and regulations under the Therapeutic Goods Administration (TGA) for genetic testing devices and medical interventions.
- New Zealand: New Zealand follows regulations under the Ministry of Health and Medical Council guidelines for genetic testing and research ethics
6. South America
- Brazil: Brazil has regulations on genetic research and testing, including guidelines from the National Health Surveillance Agency (ANVISA).
- Argentina: Argentina follows guidelines on genetic testing and research ethics, although specific legislation may vary by region.
7. Middle East
- Israel: Israel has regulations on genetic testing and research ethics, including guidelines from the Ministry of Health.
- United Arab Emirates (UAE): UAE follows guidelines on genetic research and ethical standards, although specific legislation may vary.
Summary: Regulations and laws regarding genetic testing and interventions vary widely across continents and countries. Each region may have its own legislative frameworks, guidelines, and ethical standards governing the use of genetic information in healthcare, research, and beyond. These regulations aim to ensure ethical conduct, protect patient rights, and promote public health while balancing scientific advancement and societal concerns. Staying informed about local regulations and guidelines is essential for healthcare providers, researchers, policymakers, and individuals involved in genetic testing and interventions worldwide.
NEED FOR A holistic counseling approach from pre-conception to labor: It should be multifaceted, addressing not only the medical and genetic aspects but also the emotional, ethical, and social dimensions of decision-making. By providing comprehensive education, psychological support, ethical guidance, individualized care, effective communication, legal and social information, and continuous support, counselors can empower individuals and families to make informed and considered decisions that are aligned with their values and circumstances.

- “The potential for misuse of genetic information in a society that values individualism and autonomy above all cannot be ignored.” – Eric Juengst, Bioethicist
- “True informed consent means that the patient understands the risks and benefits, but also the uncertainty inherent in genetic information.” – Julian Savulescu, Philosopher and Bioethicist
- “Respect for autonomy is paramount, but we must also consider the societal context that may influence individual choices.” – Tom Beauchamp, Bioethicist
- “The ethical landscape of genetic interventions is fraught with challenges to personal autonomy, particularly when future generations are considered.” – Leon Kass, Bioethicist and Physician
- “We must be vigilant against the resurgence of eugenic thinking, which can easily creep into the practice of genetic enhancement.” – Marcy Darnovsky, Executive Director, Center for Genetics and Society
- “The social implications of genetic interventions extend far beyond the individual, potentially reshaping societal norms and values.” – Francis Fukuyama, Political Scientist and Author
- “The relief of pain must be considered as important a principle of medicine as the relief of fever.” – Oliver Wendell Holmes, Physician and Poet
- “The use of opioids in labor must be weighed carefully, considering both maternal comfort and the potential for neonatal effects.” – American College of Obstetricians and Gynecologists
- “Respect for autonomy is the principle that underlies the practice of informed consent in medical ethics.” – Tom Beauchamp and James Childress, Principles of Biomedical Ethics
- “The patient’s autonomy is the prime value in medical ethics; paternalism is no longer acceptable.” – Edmund Pellegrino, Bioethicist
- “The physician should not only be the healer but also the comforter, counselor, and friend of his patients.” – Hippocrates, Ancient Greek Physician
- “To cure sometimes, to relieve often, to comfort always.” – Edward Trudeau, Physician and Philosopher
- “First, do no harm.” – Hippocratic Oath, attributed to Hippocrates
- “It is better to prevent a disease than to cure it.” – Pierre Fauchard, Father of Modern Dentistry
- “Justice in health care should be seen as a continuous debate, not as a final formula.” – Norman Daniels, Philosopher of Justice in Health Care
- “Justice is what love looks like in public.” – Cornel West, Philosopher and Social Critic
- “Informed consent is a process, not a form.” – Ezekiel Emanuel, Bioethicist
- “Consent is the act of granting permission, based on an understanding of what one is consenting to.” – American Medical Association
- “We do not inherit the earth from our ancestors; we borrow it from our children.” – Native American Proverb
- “Sustainable development is development that meets the needs of the present without compromising the ability of future generations to meet their own needs.” – Brundtland Report, United Nations
- “The true sign of intelligence is not knowledge but imagination.” Albert Einstein
- “The only true wisdom is in knowing you know nothing.” Socrates

“Somewhere, something incredible is waiting to be known.” Carl Sagan